Introduction: The Malignant Transformation of Melanocytes
In the hierarchy of dermatological oncology, Melanoma represents the most aggressive and clinically significant form of skin cancer. This malignancy originates within melanocytes, the specialized dendritic cells residing in the stratum basale of the epidermis that are responsible for synthesizing the protective pigment melanin. Under homeostatic conditions, melanocytes distribute melanin to surrounding keratinocytes to shield cellular DNA from ultraviolet (UV) radiation damage. However, when the genetic architecture of these melanocytes is compromised—frequently due to cumulative or acute, blistering UV exposure—uncontrolled cellular proliferation is triggered.
At Grazia Skin Clinics, we approach melanoma with a strict emphasis on early detection and multi-disciplinary intervention. Unlike non-melanoma skin cancers such as Basal Cell Carcinoma or Squamous Cell Carcinoma , which tend to remain locally indolent, melanoma possesses an inherently high metastatic potential. Consequently, if it is left unchecked, malignant cells can quickly breach the dermo-epidermal junction. From there, they invade the papillary and reticular dermis, gaining direct access to the lymphatic network and peripheral vascular channels.
Understanding the molecular triggers—such as the widely studied $BRAF$ V600E gene mutation found in a significant percentage of cutaneous melanomas—has transformed how the medical community treats this disease. Today, clinical management has evolved past simple surgical excision into a sophisticated field encompassing targeted molecular therapies, advanced immune-checkpoint inhibition, and detailed sentinel lymph node mapping.
Symptoms: The ABCDE Diagnostic Framework and Clinical Indicators
The presentation of cutaneous melanoma can be highly deceptive, often mimicking a benign acquired melanocytic nevus (common mole). Therefore, clinicians and patients must rely on the structured ABCDE diagnostic protocol to catch early structural mutations.
- A – Asymmetry: Benign moles are typically perfectly symmetrical. In contrast, if you draw a line directly through the center of a malignant melanoma, the two halves will fail to match structurally, indicating uneven, chaotic cellular growth.
- B – Border Irregularity: The margins of an early melanoma are rarely smooth or well-defined. Instead, they present with notched, scalloped, jagged, or poorly demarcated borders where the tumor cells are unevenly invading the surrounding healthy tissue.
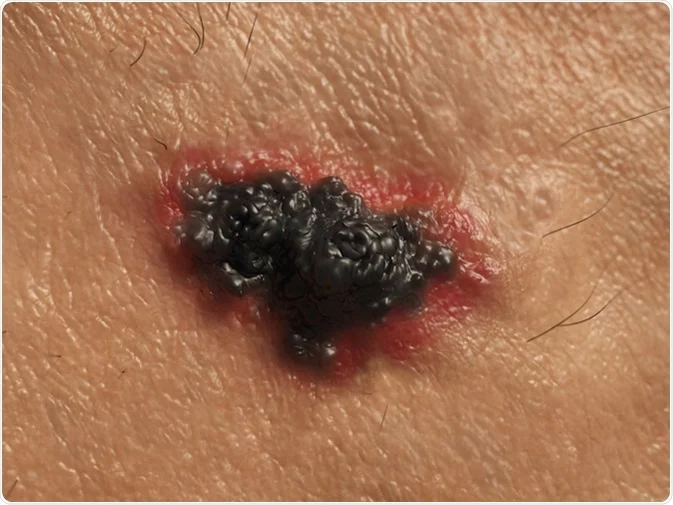
- C – Color Variegation: Healthy nevi usually display a uniform shade of brown or tan. Conversely, a melanoma frequently exhibits color variegation. Specifically, it may feature a chaotic mixture of shades, including jet black, dark brown, light tan, and even ominous areas of red, white, or blue (representing localized inflammation, regression, and deep vascularization respectively).
- D – Diameter Evolution: While benign moles usually remain stable and under (the size of a standard pencil eraser), melanomas are typically larger when diagnosed. However, it is vital to note that early-stage lesions can present at smaller dimensions, making any rapidly growing spot a clinical concern.
- E – Evolving (The Most Crucial Indicator): A healthy spot remains static over years. On the other hand, a lesion that is dynamically changing in size, shape, surface elevation, or color demands immediate histopathological evaluation. Furthermore, the sudden development of new sensory symptoms—such as localized pruritus (itching), tenderness, oozing, crusting, or spontaneous bleeding—is a clear warning sign of a changing lesion.
Classification: The Primary Histological Types of Melanoma
Melanoma is not a uniform disease; rather, it manifests in several distinct histological subtypes, each with unique growth patterns, anatomic locations, and clinical trajectories.
┌──────────────────────────────┐
│ Cutaneous Melanoma Types │
└──────────────┬───────────────┘
│
┌───────────────────────┼───────────────────────┐
▼ ▼ ▼
┌─────────────────┐ ┌─────────────────┐ ┌─────────────────┐
│ Superficial │ │ Nodular │ │ Lentigo Maligna │
│ Spreading │ │ • Aggressive │ │ • Chronically │
│ • Radial growth │ │ • Vertical growth│ │ sun-damaged │
│ • Most common │ │ • Early invasion│ │ skin (elderly)│
└─────────────────┘ └─────────────────┘ └─────────────────┘
1. Superficial Spreading Melanoma (SSM)
This is statistically the most prevalent subtype, accounting for roughly of all diagnosed cutaneous melanomas. Typically, it favors the upper back in men and the lower extremities in women.
- Growth Phase: It exhibits an extended radial growth phase, spreading horizontally along the epidermal layer for months to years before invading deeper tissues. Consequently, this provides a crucial window for early detection and curative surgical removal.
2. Nodular Melanoma (NM)
Nodular melanoma is the most aggressive subtype, comprising approximately of cases. Unlike Superficial Spreading Melanoma, it lacks a noticeable horizontal growth phase.
- Growth Phase: From its inception, it enters a rapid vertical growth phase, plunging downward into the deep dermal layers. As a result, it frequently presents as a firm, dome-shaped, dark papule or nodule that may ulcerate and bleed. It requires immediate, aggressive surgical intervention due to its rapid timeline of invasion.
3. Lentigo Maligna Melanoma (LMM)1
This variant occurs almost exclusively on chronically sun-damaged skin in elderly patients, routinely appearing on the face, neck, and forearms.
- Growth Phase: It begins as an in-situ lesion called Lentigo Maligna (an irregular tan-brown patch). It grows horizontally across the skin surface for decades. However, once the atypical melanocytes cross the basement membrane, it transitions into Lentigo Maligna Melanoma, requiring full oncological treatment.
4. Acral Lentiginous Melanoma (ALM)
This subtype is unique because its development is not driven by UV sun exposure. Instead, it appears on palmoplantar surfaces (the palms of the hands and soles of the feet) and beneath the nail beds (subungual melanoma).
- Clinical Relevance: While it accounts for a low percentage of cases in lighter skin tones, it is the most common form of melanoma diagnosed in patients with darker skin pigmentation. Because it occurs in hidden or unexpected areas, diagnosis is frequently delayed, leading to a poorer clinical prognosis.
Treatment: The Multi-Disciplinary Oncological Protocol
Modern melanoma treatment depends entirely on the Breslow Depth (the exact microscopic measurement of the tumor’s thickness in millimeters from the top of the granular layer to the deepest point of invasion) and TNM staging.
EPIDERMIS ▲ [==============] 0mm (In Situ)
──────────────────┼───────────────────────────────
PAPILLARY │ [==============] <1mm (Thin)
DERMIS │
──────────────────┼───────────────────────────────
│ [==============] 1-4mm (Intermediate)
RETICULAR │
DERMIS │
▼ [==============] >4mm (Thick / Deep)
1. Wide Local Excision (WLE)
Surgical removal remains the definitive primary treatment for localized melanoma. Specifically, the surgeon removes the primary tumor along with a safety margin of healthy surrounding skin to catch any microscopic, outlying tumor cells.
- In-Situ Melanoma: Requires a conservative clearance margin.
- Invasive Melanoma : Requires a strict margin, extending down through the subcutaneous tissue to the deep muscle fascia.
2. Sentinel Lymph Node Biopsy (SLNB)
For tumors showing intermediate thickness (generally a Breslow depth or displaying high-risk features like ulceration), a Sentinel Lymph Node Biopsy is executed alongside the primary surgery.
- The Mechanism: A radioactive tracer and blue dye are injected at the tumor site to trace the fluid pathway to the first draining lymph node (the “sentinel”). If this node is surgically removed and tests negative for cancer, the disease has likely not spread. However, if microscopic melanoma cells are detected, the patient is up-staged to Stage III, triggering systemic therapeutic protocols.
3. Advanced Immunotherapy (Checkpoint Inhibition)
For advanced, metastatic, or resected Stage III/IV melanomas, immunotherapy has largely replaced traditional chemotherapy. Essentially, these drugs unmask the cancer cells, allowing the patient’s own immune system to recognize and destroy them.
- Anti-PD-1 Antibodies (Nivolumab , Pembrolizumab): These medications block the programmed cell death protein 1 pathway on T-cells. By doing so, they prevent the tumor from sending a “turn off” signal to the immune system.
- Anti-CTLA-4 Antibodies (Ipilimumab): Works deeper within the lymphatic system to boost overall T-cell activation and proliferation. Often, it is combined with anti-PD-1 therapy for a more powerful, synergistic therapeutic effect.
4. Targeted Molecular Therapy
Approximately half of all cutaneous melanomas feature a mutation in the gene, which acts like a broken “on” switch for cell replication.
- The Protocol: Patients who test positive for this mutation can be treated with combination oral targeted therapies, such as Dabrafenib + Trametinib or Vemurafenib + Cobimetinib. Specifically, these drugs selectively shut down the mutant $BRAF$ and $MEK$ protein signaling pathways. This approach can cause rapid, dramatic tumor shrinkage in advanced stages.
Aftercare: Long-Term Surveillance, Recovery, and Photoprotection
Post-treatment care for a melanoma survivor requires life-long, meticulous surveillance. The goal is two-fold: supporting structural wound healing and monitoring for localized recurrence or secondary primary tumors.
- Rigorous Dermatological Screening: Patients with a history of melanoma face a significantly higher risk of developing a recurrence or a completely new primary skin cancer.
- Advanced Photoprotection Restructuring: UV radiation continues to be a dangerous environmental trigger for genetic mutations
- Furthermore, physical barriers like UPF 50+ clothing, wide-brimmed hats, and avoiding the sun during peak hours are vital lifestyle changes.
- Lymphatic System Monitoring: For patients who underwent a complete lymph node dissection, a condition called lymphedema can develop.
- Surgical Wound and Scar Management: Once the wide local excision sutures are removed, the site must be managed to minimize deep scar.
Conclusion: The Critical Value of Clinical Vigilance
Melanoma remains one of the most clinically challenging diagnoses in dermatology,
At Grazia Skin Clinics, our oncological mission centers on thorough diagnostic screening and educating patients on the changing patterns of their skin. By combining advanced surgical excision techniques with modern targeted therapies and immunotherapies, the medical community continues to make massive progress against this disease.
REFERENCE:-
https://www.cancer.gov/types/skin/patient/melanoma-treatment-pdq
